Vintage School 1.6
 |
| A wide variety of causes and conditions can contribute to taste or smell dysfunction including many medications, chemicals and pollutants, as well as head trauma and infection of the middle ear. |
Like our other senses, the chemical senses of taste and smell are equally susceptible to dysfunction - either sense can be diminished, heightened, distorted or even completely absent. These ailments have been classified as "-osmias" (smell disorders) and "-geusias" (taste disorders). Such disorders can be total (all odours or tastes), partial (affecting several odours or tastes), or specific (only one or a select few odours or tastes). We will refer to one or another of these conditions throughout our study of the senses. They are defined as follows:
*Anosmia- an inability to detect odours
*Hyposmia- a decreased ability to detect odours
*Dysosmia- a distorted identification of smell
- Parosmia- an altered perception of smell in the presence of an odour, usually unpleasant
- Phantosmia- the perception of smell without an odour present*
- Agnosia- an inability to classify or contrast odours, although able to detect odours
* Ageusia- an inability to taste
* Hypogeusia- a decreased ability to taste
* Dysgeusia- a distorted ability to taste(1)
* Heterogeusia- Inability to distinguish between tastes
* Cacogeusia- a bad taste in the mouth that does not go away
There are actually a large and varied range of causes and conditions leading to these seemingly bizarre disorders, which afflict a significant proportion of the population. Indeed, this inventory of causes and cautions was first compiled when my own experience with smell disorder prompted me to investigate the subject further. I came to realise that the scope and variety of these disorders must go some way to accounting for individual differences in the perception of flavour.
Smell Disorders
Disturbances in olfaction can result from pathologic processes at any level along the olfactory pathway. Usually this occurs because transmission of an odorant stimulus to the olfactory neuroepithelium is disrupted, or because of sensorineural defects (i.e.- lesions or disease in the inner ear or the auditory nerve). But overall, the most common causes are nasal and/or sinus disease, head trauma or a prior viral upper respiratory infection.
1. Conductive defects
o Inflammatory processes cause a large portion of olfactory defects. These may include rhinitis of various types, including allergic, acute, or toxic (eg, cocaine use). Chronic sinus disease causes progressive mucosal disease and often leads to decreased olfactory function despite aggressive allergic, medical, and surgical intervention.
o Masses may block the nasal cavity, preventing the flow of odorants to the olfactory epithelium. These include nasal polyps (most common) and any malignancy.
o Patients with laryngectomies or tracheotomies experience hyposmia because of a reduced or absent nasal airflow.
2. Central/sensorineural defects
o Infectious and Inflammatory processes contribute to central defects in olfaction and in transmission of odours. These include viral infections (which may damage the neuroepithelium), sarcoidosis (affecting neural structures), Wegener granulomatosis, and multiple sclerosis.
o Congenital causes may be associated with neural losses. Kallman syndrome, for example, causes anosmia (inability to detect odours) due to the failed proper development of the olfactory structure from the earliest stage to maturity.
o Endocrine disturbances affect olfactory function (eg, hypothyroidism, hypoadrenalism, diabetes mellitus).
o Head trauma, brain surgery, or subarachnoid hemorrhage may stretch, damage, or cut across the delicate fila olfactoria and result in anosmia.
o Toxicity of systemic or inhaled drugs (eg, aminoglycosides, formaldehyde) can contribute to olfactory dysfunction. Many other medications and compounds may alter smell sensitivity, these are discussed below.
o Nutritional deficiencies have been found to affect olfaction (eg, vitamin A, thiamine, zinc).
o Degenerative processes of the central nervous system (eg, Parkinson disease, Alzheimer disease as well as normal aging) have been found to cause hyposmia (a decreased ability to detect odours). In the case of Alzheimer disease, olfactory loss can be the first symptom.(2)
Taste Disorders
Much of what is perceived as a taste defect is truly a primary defect in olfaction, which alters flavour. Other than smell disfunction, some frequent causes of taste disfunction are as follows:
* Lesions at any site from the mucosa, taste buds, unmyelinated nerves, or cranial nerves to the brain stem may impair taste.
* Oral cavity and mucosal disorders including oral infections, inflammation, and radiation-induced mucositis can impair taste sensation. The site of injury with radiotherapy is probably the microvilli of the taste buds, not the taste buds themselves, since taste buds are thought to be radioresistant.
* Poor oral hygiene is a leading cause of hypogeusia (a decreased ability to taste) and cacogeusia (a bad taste in the mouth). Viral, bacterial, fungal, and parasitic infections may lead to taste disturbances because of secondary taste bud involvement.
* Malignancies of the head and neck, as well as of other sites, are associated with decreased appetite and inability to appreciate flavours.
* Use of dentures or other palatal prostheses may impair sour and bitter perception, and tongue brushing has been shown to decrease taste acuity.
* Surgical manipulation may alter taste permanently or temporarily by altering airflow, decreasing taste perception or decreasing the number of taste buds.
* Nutritional deficiencies are involved in taste aberrations. Decreased zinc, copper, and nickel levels can correlate with taste alterations. Nutritional deficiencies may be caused by anorexia, malabsorption, and/or increased urinary losses.
* Hormonal fluctuations in menstruation and pregnancy also influence taste.
* Direct nerve or Central Nervous System damage, as in multiple sclerosis, facial paralysis, and thalamic or uncal lesions, can decrease taste perception.
* Many other diseases can affect gustation (eg, lichen planus, aglycogeusia, Sjögren syndrome, renal failure with uremia and dialysis, geographic tongue and cirrhosis).(3)There is also an unexpected relationship between the ear and tongue which can result in a significant taste disorder. The chorda tympani nerve travels behind the tympanic membrane through the middle ear on its path from the tongue to the brain. Infection of the middle ear(Otitis Media) reduces one's ability to hear and consequently to taste so that both Sonata and Shiraz become indiscernible - a doubly cruel blow.
But eliminating the impaired detection of potentially dangerous smells like smoke from house fire, gas leaks or spoiled food, taste and smell disorders, on the whole, do not appear as serious complaints as cancer or heart disease. Lucinda Miller, Pharm.D., in the division of family medicine at the Baylor College of Medicine in Houston adds that this attitude translates into skimpy research funding. Further frustrations stem from the fact that the physical bases of the chemical senses are difficult to study in a laboratory. Taste buds, for example, cannot easily be grown outside of the body, as can visual tissue such as rod and cone cells. And, more often than not, laboratory animals cannot stand in for humans because their tastes differ. With regard to sugars, for example, humans love sucrose (table sugar), but armadillos, hedgehogs, lions, and sea gulls do not respond to it. Opossums love lactose (milk sugar) but rats avoid it, and chickens hate the sugar 'xylose', while cattle love it and we're indifferent. (At least such diverse tastes in the animal kingdom ensure that there is enough food to go around).
Further funding for research seems warranted by statistics: More than 250,000 Americans visit their physician every year because of chemo-sensory problems and studies have found that 66% of people are aware of a period in their life when they experienced decreased smell acuity.(4) Perhaps the main obstacle remains the difficultly of comprehending just how profoundly one's enjoyment of life can be affected by a chemo-sensory loss. One sufferer, after spending a year sneezing for no apparent reason, was suddenly unable to smell or taste. For years, she lived on her memories of smelling hot coffee and freshly peeled oranges. Her condition, attributed to"allergy and infection,"mysteriously came and went. When taste and smell were intact, she rushed off to the nearest restaurant, but more often than not, her sensory acuity had faded before the food arrived. After countless blood and urine tests, CAT scans, and biopsies, she resorted to having her sinuses drained, and took zinc supplements. Nothing worked. Finally, she found relief with prednisone. This strong steroid drug reduces swelling of the mucous membranes in the nose, and may therefore improve the sense of smell, but its efficacy as a treatment for smell disorders has not been proven. Feeling better, the woman went about smelling everything- "I inhaled all odours, good and bad, as if drunk".(5)
"People with a smell or taste disorder really have a lower quality of life," says Dr. Gary Beauchamp, director of the Monell Chemical Senses Center in Philadelphia. "They can't fully enjoy the simple aspects of normal life, like eating and drinking [which] may be one of the few pleasures they have." Anxiety and depression, as well as anorexia and nutritional deficiencies often result.(6) The impact of smell and taste dysfunction should not be underestimated.
Adults over the age of 60 are most prone to chemo-sensory faults. The sense of smell which is most dramatically impaired with aging. Research suggests a loss of 1% for every year of one's life, so that at age 50, for example, one's ability to perceive smells has been reduced by 50%. A study comparing the ability to detect ethyl mercaptan, an ingredient in liquid petroleum gas, showed that adults age seventy-four required ten times more of the chemical to detect it than did twenty-year-olds. However, the ability to detect odours varied across older adults, with some performing as well as younger subjects. Other studies have consistently shown that older people find it more difficult than younger people to identify sweet, bitter and salty tastes, or to distinguish differences in concentration of these tastes. The gradual decline in taste and smell usually becomes noticeable by age 60 and continues past the age of 70. "No one really knows why we lose these senses," says Monell's Marcia Pelchat, Ph.D. "One theory is that the cells in the nose aren't replaced as efficiently. As with hearing loss, however, it may not occur in everyone."
The Effects of Chemicals & Pollutants on Smell & Taste
While smoking tobacco is probably the most concentrated form of pollution that most people will ever be exposed to, a broad range of chemicals have being identified as affecting the upper alimentary and respiratory tracks, generating asthma-like conditions as well as unpleasant odour and taste sensations. In the same way that a cigar or cigarette dampens our sense of smell, exposure to toxic chemicals like benzene, benzol, butyl acetate, carbon disulfide, chlorine, ethyl acetate, formaldehyde, hydrogen selenide, paint solvents, sulfuric acid and thrichloroethylene, as well as exposure to industrial agents like ash, cadmium, chalk, chromium, iron carboxyl, lead, nickel and silicone dioxide, can damage the olfactory system causing anosmia or hyposmia. One case documented described how, "a 45-year-old woman suddenly found that once-pleasant smells had become offensive. Her doctor...traced her problem to inhaling a paint stripper. Hydrocarbon solvents in the product - tolune, methanol, and methylene chloride - were the culprits responsible for her "cacosmia," the association of an odor of decay with normally inoffensive stimuli."(7)
Other chemicals that have been found to cause damage to the olfactory system include those found in insecticides, soil fumigants, herbicides and fungicides including:
2 - carbofuran
3 - chlorpyrifos
4 - chlorpyrifos oxon
5 - demeton
6 - malathion
7 - meth amidophos
the carbamate insecticides
1. . carbaryl
2. . pyrethroid fenvalerate
& the herbicides
1. . paraquat
2. . glyphosate
Such chemicals can significantly alter (both reduce and enhance) the pattern of electrophysiological activity in tasters. The alterations in taste are probably due to changes in metabolic activity in taste cells or levels of neurotransmitters, rather than modification in the transduction system. The impact of these pollutants on the olfactory system must be of some concern to agricultural workers and vignerons alike, (as well as neighbouring residents.) One cannot over stress the precautions which ought to be taken with chemicals in the field and their potential impact on fellow workers and consumers down the food chain. Rate of application, oversprays and pollution of waterways are all issues of universal concern that can impact upon our ability to smell and taste.
Drugs & Distortions
In a related experiment, Schiffman et al (1998) observed how oral exposure to six psychotropic drugs (amitriptyline HCl, clomipramine HCl, desipramine HCl, imipramine HCl, doxepin HCl, and trifluoperazine HCl) altered taste perception of other compounds such as NaCl and sucrose. The results indicated that both hypogeusia (decreased ability to taste) and dysgeusia (distorted ability to taste) could be induced by psychotropic medications.(8)
However, these distortions were not only caused by drugs of the psychotropic kind:"A group of 12 travelers touring Peru and Bolivia prepared for a day of hiking in the Andes mountains. A day before, three of them had begun taking acetazolamide (Diamox), a drug that prevents acute mountain sickness, which each had previously suffered. The headache, nausea, weakness, and shortness of breath of acute mountain sickness typically begins when one reaches 5,900 feet elevation, and can progress to severe respiratory problems by 9,000 feet. These hikers planned an expedition to 12,000 feet. All went well, but the night after the climb, the group went out for beer. To three of the people, the brew tasted unbearably bitter, and a drink of cola to wash away the taste was equally offensive. At fault: acetazolamide. The taste distortion caused by this particular drug makes biochemical sense. The drug inhibits an enzyme that normally dismantles bitter-tasting carbonic acid before it has a chance to register on the taste buds". (9) In fact, the drug distorts the taste of anything with carbonation, enabling the person to experience the terribly bitter taste of carbonic acid.
Other drugs notorious for distorting taste include the anti-inflammatory drug penicillamine, the anti-hypertensive captopril (Capoten), and transdermal (patch) nitroglycerin to treat chest pain. (See table below) The antibiotics tetracycline and metronidazole (Flagyl) cause a metallic taste.
|
Antibiotics Anticonvulsants Antidepressants |
Antihistamines and Antihypertensives and
|
Anti-inflammatory agents Antimanic drug Antineoplastics Antiparkinsonian agents |
Antipsychotics Antithyroid agents Lipid-lowering agents Muscle relaxants |
Philadelphia, Pennsylvania. Columbia-Presbyterian Medical Center, New York, New York. http://www.aafp.org/afp/20000115/427.html
Finally, chemotherapy and radiation treatment, especially to the head and neck areas, also inhibit (but sometimes enhance) both taste and smell. The main cause of taste deficit resulting from these therapies is believed to be due to the disappearance of or damage to taste buds and damage to the salivary glands. Thankfully, our taste bud cells are in a constant state of flux. They replace themselves on average every 10 days well into late middle age, after which, as with most of life's afflictions, age itself becomes the ultimate check to indulgence. For those already facing this predicament, we conclude with some suggestions that might go some way to relieving the situation:
Avoid overexposing your taste buds to any one sensation. It can temporarily deaden your sensitivity. For example, excess coffee can numb the sensitivity to bitter tastes.
Wait 10 to 15 minutes after brushing your teeth. Lauryl sulfate, a compound in most toothpastes, can trigger a drop in taste sensitivity.
Include a variety of textures in your meals. Texture can sometimes help compensate for a loss in taste and smell sensitivity.
Avoid eating food that is very hot or very cold; flavours are less intensely sensed at temperature extremes.
Stop smoking. Eat slowly to savour the flavours and aromas of food. If you enjoy wine, then drink more perfumed, full flavoured styles - the kind which Australia produces in abundance.
Switch from one food to another several times during a meal. Even under normal conditions, taste buds become desensitized to flavours. Alternating helps "wake them up." (10)
Taste Blindness & Supertasters
Amongst the characteristics that make each of us unique are our differences in taste that go beyond a penchant for self-indulgence. In the early twentieth century, the characteristic of taste sensitivity as an inborn trait became the focus of science and a picture began to emerge of vastly dissimilar tongues sensing the same world, only very differently. This picture was inspired by an unusual twist of fate and developed from an observation by an industrial chemist, Arthur L. Fox.
Between 1931 and 1932, Fox, working at the DuPont Co. Delaware, was researching the relationship between chemical constitution and taste. At the time, Fox was working with the compound 'PTC' (Phenylthiocarbamide) when the substance accidentally scattered into the air. A colleague who inhaled the PTC dust commented on the terrible taste, but Fox couldn't taste anything. He went on to test a variety of his associates and discovered that some experienced PTC as intensely bitter, while others said the compound "has no more taste than sand".(11)This discovery suggested to Fox that, at least as far as PTC was concerned, people could be divided into two groups: tasters and non-tasters, or that some people could be partially taste 'blind'.
Fox reported the findings later the same year in Science News and handed out crystals of PTC at the 1932 A.A.A.S. meeting, asking how many passers-by could taste it. About a quarter of the people were nontasters, while everyone else said PTC was bitter. His discovery activated geneticists to begin evaluating families for their distribution of apparent taste blindness. After two family studies, researchers concluded that an ability to taste PTC was an inherited trait, produced by a dominant gene allele t. Those with one dominant and one recessive allele (ie. tT or Tt) or people who have two dominant alleles (TT) were called 'Tasters'. On the other hand, individuals with two recessive alleles (tt) were found to be 'blind' to the taste of PTC and were labelled 'non-tasters'.
 |
| Prof. Linda Bartoshuk |
The subject might have remained a scientific curio, unless a research team led by Professor Linda Bartoshuk at Yale, Connecticut during the 1970's had decided to re examine the question asking:"What difference does it make in everyday life if someone is a taster or a nontaster of PTC?"Due to concerns about the toxicity of PTC, Bartoshuk began a supra-threshold taste study using a chemical compound PROP (6-n-propylthiouracil - a thyroid medication) as a substitute. Like PTC tasting, reactions to PROP were inherited. The scientists thought that the two tests revealed the same trait. As time went on, Bartoshuk, began to notice that a subset of people seemed unusually attuned to the bitter taste of PROP.
While the majority found PROP to be only moderately bitter, a minority found PROP to be intensely or even excruciatingly bitter. Subjects in the latter category also perceived the greatest sweetness from sugars (but not aspartame), the greatest bitterness from other bitter compounds and the greatest oral burn from ethyl alcohol and from capsicum.
Later results supporting the PROP experiments showed an association between the perceived intensity of PROP and the number of taste pores. The results turned out to be predictable: Those who found PROP the most revolting had the greatest density of fungiform papillae and taste buds; Medium tasters next, and non tasters the lowest number. From these results, Bartoshuk took Fox's notion of taste blindness one step further, but in the opposite direction. In 1991 she coined the term "Supertaster" after identifying the group of subjects whose taste buds were so numerous & dense and therefore hyper-sensitive. Each taste bud feeds information into two types of nerves: One, the chorda tympani, a branch of the facial nerve, sends taste signals to the brain for processing. A second, the trigeminal nerve, senses pain, temperature and touch.''This is really critical,'' says Dr. Bartoshuk. ''It tells us that supertasters are superfeelers and superpain-perceivers, at least with their tongues.'' (12)
| A Simple Experiment : Obtaining your own Fungiform papillae count & testing for PROP sensitivity 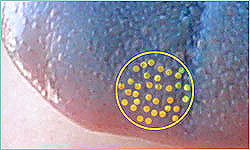 If you're curious to find out whether you are a supertaster, a non taster or somewhere in between, you don't necessarily need PROP to find out. Because PROP is a prescription drug, veteran taste researcher, Professor Linda Bartoshuk has devised a simple way of measuring the density of your own taste buds, outlined below. This is an experiment that could be done in a science lab or classroom as well as used for research. You need a template that can be placed on tongues in a consistent manner. For example, you can use a paper punch to make a hole in a 1 inch square of wax paper or you can use the reinforcements sold for notebook paper (plain paper tends to disintergrate). Either of these will give you a hole about 6-7 mm in diameter. Place the template on the tongue so that the hole is in a standard position (see picture below).  Swab blue food colouring on the front part of the tongue then move your tongue around your mouth until it is covered. Don't plan on meeting anyone important afterwards as your tongue will be a vibrant turquoise. Using a flashlight and a magnifying glass, count the number of fungiform papillae. Photographing the area is even easier. The sketch below shows examples of a supertaster and a nontaster. The circles correspond approximately to the hole produced by a typical paper punch or to the hole inside a notebook paper reinforcer. Those with 4-6 fungiform papillae spots inside the whole-punch ring are considered non-tasters. If you can count more 20-25 papillae , you are potentially a supertaster, while those in between these numbers are medium tasters.  Above: Supertasters have more papillae that are very closely arranged and smaller in size.Non tasters have fewer papillae that are loosely arranged and larger in size. The Prop test procedure as described by Linda Bartoshuk, Yale University School of Medicine. You will have to source PROP (6-n-propylthiouracil) (pharmaceutical grade). PROP is a prescription medication used to treat Grave's Disease (hyperthyroidism), designed to reduce the thyroid's ability to produce hormones. People taking this medication might take 50 mg (3-4 tablets each) daily. Each PROP paper contains about 1.6 mg PROP. Follow the procedure below for preparing PROP papers. The PROP papers are made on filter paper (Whatman #1). Heat tap water to near boiling and then add 5 grams PROP to 500ml water. The aim is to make a saturated solution. (As the solution cools, crystals will precipitate out of solution.) Dip the pieces of filter paper in the PROP solution so that they are completely soaked. We use small pieces of filter paper (3 cm circles) and allow them to dry individually on sheets of aluminium foil. The PROP crystallizes into the filter paper. Thus the paper is a convenient way to deliver a few crystals of PROP to a subject. To taste the paper, put the whole piece in your mouth and let it get well moistened with saliva. The bitter taste may build slowly or may be perceived immediately. [Those who are sensitive to the compound usually grimace like a baby as their tongue "...thrashes around their mouth like a hooked fish convulsing on the deck of a boat" (14) while non-tasters wonder what the fuss is about - it will literally taste like a piece of paper to them. -ed.] |
During the 1990's, enough data accumulated to confidently declare that approximately 25% of the American population are born 'super-tasters', a group with an unusually high number of taste buds; 25% are said to be non-tasters and 50% medium tasters. However, these numbers can vary depending upon ethnicity and sex. For example, people from Asia, Africa and South America are more likely to be supertasters, so are women. The evolutionary advantage of supertasting is unclear, but as we have conjectured in previous chapters, a heightened taste response to bitterness could represent an important advantage in avoiding toxic substances. Similarly, a pregnant woman with anything other than an acute taste and smell sensibility might prove fatal to the fetus. Once the child is born, the mother must continue to ensure that toxic food and drink does not pass through her system which would pass onto the young infant suckling**. Bartoshuk says that studies suggest that monthly estrogen fluctuations alter PROP sensations in younger women so that the sense of bitterness in foods varies throughout each month. And during the first trimester of pregnancy, even nontaster and medium-taster women find many previously acceptable foods, like coffee, to be suddenly unpalatable(13). Conversely, in our modern, energy-rich environment, supertasting may be cardioprotective, due to decreased liking and intake of fat, but may increase cancer risk via decreased vegetable intake.
Bartoshuk, who is probably now the world's leading expert on super tasters, continues to investigate whether dietary choices made by supertasters have any impact on disease patterns. In a preliminary study of colon cancer patients, she has learned that they are more likely to be super tasters. The number of cancerous polyps found was related to the extent that they perceived bitterness.
Several years ago, researchers also finally confirmed Fox's intuitions, formally identifying the two dominant alelles for the gene responsible for PROP/PTC sensitivity, known as TAS2R38, but to complicate the matter, it is also known that some people who are highly sensitive to PROP have only one.
The Tongue of a Supertaster
When it comes to sweet tastes, supertasters find many sugary foods to be sickeningly sweet, while at the same time being hyper sensitive to bitterness, and to astringency in general, finding all sorts of vegetables overly bitter, especially brussel sprouts, cabbage brocolli and kale as well as other foods like coffee, grapefruit and dark chocolate.
Acidity and the burning sensations generated by high alcohol, and spices like ginger or capsicum, also deliver an increased sensation of oral burn or pain. Hence, super tasters tend not to enjoy spicy foods. For similar reasons, food is usually preferred served tepid rather than hot.
Supertasters are extremely sensitive to gradations in fat. As fat content increases, they perceive more creaminess reacting to its mouthfeel."Fat molecules literally press against the taste buds, producing a tactile sensation that is interpreted by the brain as viscous, slippery or greasy." (15)
Other items which may also show altered patterns of preference and consumption include tonic water (quinine being more bitter to supertasters) and olives (from which the salt taste is more intensely experienced).
Given 'supertasters' possess such highly sensitive palates, does it necessarily follow that they then have superior palates? Is sensibility of taste itself sufficient for being an 'ideal' critic? Are all professional wine judges and sommeliers, for example, supertasters?
After considering the supertaster's profile, American wine critic, Mike Steinberger asked this very question: "Does being a supertaster actually help to evaluate wine?" In a three part article focusing on the physiology of the wine critic, he concluded that"...to the degree that it matters at all, it is probably more of a liability for a wine critic [to be a supertaster] than an asset"(16). He cites Gary Pickering, a professor of oenology at Canada's Brock University, who says supertasters "probably enjoy wine less than the rest of us since they have such an intense reaction to wine's astringency, acidity, bitterness and the sensation of heat from the alcohol... this combination may make wine - or some wine styles - relatively unappealing"(17).
If super-tasters,"live in a 'neon world' of taste, while non tasters are in a pastel world"(18),their opinions as wine critics might not be of much value except to other supertasters who would appear to be in the minority."The world is built for regular tasters"says Bartoshuk, and"From a purely demographic standpoint, the ideal wine critic would be a low sensitivity taster" says Steinberger, since Caucasian males, 35% of whom are nontasters, are the largest wine-buying demographic group. Tim Hanni, M.W. who unexpectedly gave out PROP tests at the Institute of Masters of Wine Sixth Symposium held in Napa Valley 2006, supsects that some of the more prominent wine critics are probably low sensitivity tasters given their fondess for heavily extracted, high alcohol wines.
The non taster / taster / supertaster debate has certainly generated some controversy amongst professional wine critics. Following the Napa Valley Symposium, U.K. M.W., Jancis Robinson, reported that "Mark Squires' bulletin board on www.erobertparker.com started a thread on whether biology determined tasting ability, initiated by someone who seemed to understand the issues and pointed out it was quite brave of me [Robinson] to admit to being anything other than normal. But that misleading prefix "super" does a lot of damage. Robert Parker himself jumped in early to declare that he couldn't abide spicy food in any form. (I like it, incidentally.) [Previously, Mr. Parker had ascribed his tasting acuity in part to having unusually deep crevices in his tongue.] (19) Then another American wine writer...dashed off a column for...the New York Sun, making me the prime perpetrator of "an almost desperate attempt by some of today's wine tasting potentates to bolster their credibility by suggesting a physical superiority." This was the last thing I was attempting."(20)
It would appear that the controversy has mainly stemmed from impulsive responses based upon an incomplete understanding of the physiology of the supertaster or the fact the word itself is something of a misnomer***. Matt Kramer sums up the confusion,"Suggesting a linkage of taste buds to wine judgment is like confusing eyesight with insight. Otherwise, Ted Williams - with his legendary 20-10 vision - would be renowned today as an art critic". (21)
As with almost any discussion concerning smell and taste, there are other contingencies:
Namely, that taste preferences are influenced by more factors than fungiform papillae count and genetic inheritance alone. (See "The Development of Taste Preferences").
That taste as opposed to smell plays a relatively minor role in the assessment of flavour, so diminishing the significance of the non taster / taster / supertaster trichotomy. (Refer to the chapters on the mechanics of smell and taste).
That the assessment of flavour can be influenced by perception and education and it is the brain which provides us with the final, unified tasting experience. (See the chapter "Perception & Persuasion.")
These issues have been approached in other chapters of this course and we encourage readers to gauge the further complexities.
Footnotes & Bibliography
* Sometimes a foul taste can persist with no food involved. This is a "taste phantom," a sensation that comes out of nowhere, says Professor Linda Bartoshuk of Yale University. The condition is fairly common among women past menopause. Bartoshuk helps pinpoint the source of phantom tastes. "Is it caused by a molecule in the mouth that shouldn't be there, or is brain stimulation abnormal? We can tell the difference by using anesthesia, which is a nerve inhibitor," she says. If she anesthetizes the mouth and the bad taste goes away, then it's due to molecules there. If, following anesthesia, the patient gets worse, this points to the brain as the cause of the problem.
** (Indeed, the figurative expression "Mother's Milk" is often used to describe the purest, most satisfying form of a drink).
*** "hypertaster" might be a more accurate and less emotive term as Jancis Robinson has suggested.
1. Disorders of Taste and Smell, Donald A Leopold, MD et al. Clinical Professor; Dept. of Medicine, Professor and Chair, Department of Otolarynology-Head & Neck Surgery, University of Nebraska Medical Center, June 2006.
2. Ibid
3. Ibid
4. Ibid
5. When Smell and Taste go Awry. Lewis, Ricki. FDA Consumer. November 1991
The woman's story appeared in the March 1988 edition of Newsweek magazine.
Ricki Lewis, a writer in Scotia, N.Y., has a Ph.D., in genetics and is the author of a college biology text.
6. Smell, Taste Disorders, Mary Sullivan, Nih Record, Vol. LVII, No 17. August 2005
7. When Smell and Taste go Awry. Lewis, Ricki. FDA Consumer. November 1991
8. Effect of Psychotropic Drugs on Taste Responses in Young and Elderly Persons. Annals of the New York Academy of Sciences 855:732-737 (1998) SUSAN S. SCHIFFMANa, BREVICK G. GRAHAM, MARK S. SUGGS AND ELIZABETH A. SATTELY-MILLER
9. When Smell and Taste go Awry. Lewis, Ricki. FDA Consumer. November 1991
10. Adapted from "How to revive your taste buds when taste and smell wane"
Environmental Nutrition, Feb, 1993 by Janet Lepke, 1993 Belvoir Media Group.
11. The Fly in the Ointment: 70 Fascinating Commentaries on the Science of Everyday Life (Joe Schwarcz). ECW Press: Toronto, Ontario, 2004.
12. Chocolate Lover or Broccoli Hater? Answer's on the Tip of Your Tongue, By Sandra Blakslee, The New York Times Science Section, February 18, 1997
13. Ibid.
14. Do You Taste What I Taste, The Physiology of a Wine Critic, Mike Steinberger, Slate Magazine June 2007
15. In an experiment, Dr. Duffy asked people to taste different milk samples -- skimmed, 1 percent fat, 2 percent fat, 4 percent fat, half and half, heavy cream and cream with oil added. Nontasters could not tell the difference between skim milk and the heavy creams, she said. Supertasters were extremely sensitive to gradations in fat. As fat content increased, they perceived more creaminess. As quoted from: Chocolate Lover or Broccoli Hater? Answer's on the Tip of Your Tongue, By Sandra Blakslee, The New York Times Science Section, February 18, 1997
16. Do You Taste What I Taste, The Physiology of a Wine Critic, Mike Steinberger, Slate Magazine June 2007
17. Ibid, as quoted from "Wine Science" by Jamie Goode, Mitchell Beazley, 2005
18. From "Supertaster" to the Taste-Blind. By Christian Boboila, Yale Scientific Magazine, Summer 2004. Pages 16-17
19. Do Taste Buds Make The Wine Critic? by Matt Kramer, The New York Sun, July 19, 2006
20. Stick out your tongue to see if you're a 'hypertaster', Jancis Robinson, San Francisco Chronicle, Friday, December 15, 2006
21. Do Taste Buds Make The Wine Critic? by Matt Kramer, The New York Sun, July 19, 2006
Other References: Susan S Schiffman, Mark S Suggs, Mohamed B Abou, Donia Robert Perickson and H Troy Nagle. Department of Psychiatry, Pharmacology and Psychology. Duke University Medical Center, Durham. Dept of Electrical and Computer Engineering North Carolina State University. Pharmacology Biochemistry and Behaviour, Vol 52, No. 1, pp 189-194, 1995